The school year is progressing along lickety split! We’ve been back to school for 94 days and have 197 left until summer break… including weekends and holidays…not that I’m counting or anything like that. Allergies…CHECK! Immunizations…CHECK! Vision screening… CHECK! What’s next? Follow-ups for sure (with puberty class lingering). You can tell I am a school nurse for elementary school students. Maybe next year I will look at a change and see about middle school or even high school. But wait! I digress…let’s talk about vision screenings.
This is a long article…and Nurse Kevin does a lot of gabbing…if you want to scroll down to see the ailments we are looking for during vision screening, feel free. But, take note: It will hurt my feelings if you miss my rambling…
Na! We’ll digress a bit more…
I remember way back in Army basic training (1998), one of the first things they did to us were all kinds of medical exams There we were all in a line and sporting nothing but our olive-green government-issued briefs (boxers for those who felt they needed a bit more *room*). We were lined up one-by-one to get shots…with this gun-lookin’ injection apparatus. Wait! Did they change that needle? There we were, walking through an immunization assembly line with nothing on but our green BVDs and with both deltoids dripping blood and leaking this clear liquid (immunization juices) from multiple injection sites.
We were ushered along to declare our religious preferences for our dog tags and then to sit on a cold, plastic seat for vision screenings. Getting up from those seats was like having flesh ripped after our bare thighs had stuck to the plastic surface. I remember how my new Velcro wallet sounded when I opened it…yeah…it was a lot like that.
Nothing about the findings of our medical exams were discussed with us. I guess my vision screening went okay; I was one of the lucky ones that didn’t get a pair of those thick black-rimmed glasses like a dozen or so of my fellow soldiers received…and at a complete surprise to many of those in the new vision-impaired club. And what do you think happened to those glasses the first chance those 17- and 18-year-old soldiers got? Yep! Afte rall, it’s kinda hard to think you have perfectly good vision your whole life and then be told to wear the new glasses in an already stressful environment.
WOW! What efficiency! Mass immunizations, health exams, vision and hearing exams, and then out the door to get into formation for the day’s instructions…school systems should take notice…and I am only a little kidding…
Vision screenings
Each year I screen my kindergartners and my third-graders. While I have the equipment, I send out a school-wide message asking the teachers of other grades to provide a name or two of children they’ve notice having difficulty, and I will screen them as well in order to rule out vision issues. Often, based on teacher concerns, I am able to identify an issue that needs to be addressed with an ophthalmologist (eye M.D.) or optometrist.
Review of abbreviations
It’s not surprising that the abbreviations for the medical documentation of the eyes is confusing. There are actually dozens and dozens of abbreviations for the eyes and for conditions of the eyes. But, we school nurses will not be assessing for things like pseudoexfoliation glaucoma, non-arteritic ischemic optic neuropathy, or epidemic keratoconjunctivitis. So, knowing what PXG, NAION, and EKC mean may be a waste of brain bandwidth. But, we do need to know these three for sure:
Oculus dexter (right eye) (OD)
Oculus sinister (left eye) (OS)
Oculus uterque (both eyes) (OU)
For me, I’d just as soon document right, left, and both or bilateral — especially in the school house. There ain’t too many mammas, daddies, or teachers that know what OU, OS, or OD mean. Now, with that being said, I do document “PERRLA.” That’s ‘cause I am too doggone lazy to type out, “Pupils equal, round, reactive to light and accommodation.”
First of all, how do we see?
We all agree that seeing is a pretty awesome deal. I do like to see stuff. We are able to “participate” in the world by the five senses: touch, taste, hearing, smell, and sight. I am not sure how you feel, but of these senses; I think sight is my favorite (I do a lot of photography). Touch is pretty cool. Taste…well…my tight 34s may have something to say about that. Hearing…pretty cool. But, well…did you ever see the movie “Up” when he turned down the hearing aid? Smell is nice…but then again I live with a 12-year-old boy. Yes, I would have to say sight is my favorite.
You don’t actually “see” the object you are looking at. Light is seen either as direct light or indirect light. The phone, tablet, or computer monitor you are looking at is direct light. Your hands on the keyboard or holding the phone or tablet are “seen” due to the direct light hitting the skin, sleeves, rings, fingernail polish, and the like. The direct light becomes indirect light and reflects off the surface and in the color from which the light was reflected. In a pitch-black room, you would not see your hands; they give off no light. But, when the lights are on, the light source (direct light) strikes your hands and the light “bounces” back and into (literally) your eyes.
The light travels through the iris (the colored part of the eye) and into the pupil (the dark center of the eye). Then the light travels through the lens and is “bent” to a pin point. It’s at that exact, sharp point where the light “should” hit the retina (the “film / digital sensor” of the eye).
The basics of the eye could be described like the basics of a camera…only awesome-er! The light enters the eye through the lens, is bent at an angle, flips upside down, and then strikes the surface of the eye at a fine point…normally.
Most children in your school “see” just fine. But, for those children with undiagnosed vision issues, learning will be much, much more difficult. After all, about 80% of the information presented in the classroom is learned visually. Children with vision issues will either have perception issues (“understanding” what you see) or they will (more likely) have issues with functional vision. Issues with “functional vision” are what we school nurses can identify.
Understanding the findings (FINALLY!)

I do a vision screening (not a vision exam). That’s important…well…it’s not all that important to me. But I, as the school nurse, do a screening. The doctor does the examining. The vision screening we do looks for these common issues:
- Myopia (nearsightedness)
- Hyperopia (farsightedness)
- Astigmatism (blurred vision)
- Anisometropia (unequal refractive power)
- Strabismus (eye misalignment)
- Anisocoria (unequal pupil size)
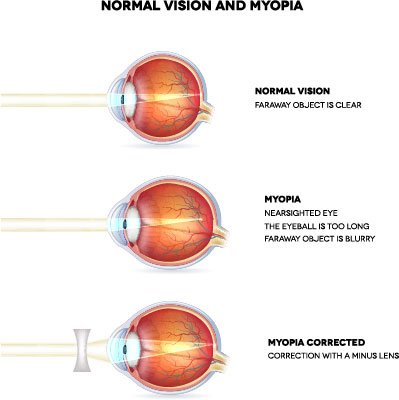
Myopia (nearsightedness)
At almost 50 years old, I have come to the determination that most of the population of the globe have myopia… “myopia” in the literary meaning.
The medical condition of myopia has a similar meaning, yet instead of lacking in intellectual sharpness, the person is suffering from visual sharpness. Remember that focal point we talked about earlier. In myopia or nearsightedness, the focal point falls in front of the retina (somewhere in the middle of the eye). This results in objects that are far away appear blurry. What is “far away?” Depends…very subjective…
If the visual image reaches the sharp focus point in front of the retina the eye it may be due to the eye not be “round.” The eye may be more oval like an egg laying on its side. A “longer” eye “pushes” the retina back a bit. So, the physical length of the eye is greater than the optical length. This may happen in the school-aged years during a period of rapid growth and may resolve later in life (or maybe not).
Hyperopia (farsightedness)
In contrast to myopia, hyperopia could also be due to an oval eye but instead of resembling an egg lying flat, it would resemble an egg standing upright. This would cause the retina to be closer to the lens. The light entering the eye does not have “room” for the length of the sharp focal point to reach the retina and objects that are closer to the eye appear blurry.
Like myopia, the person is suffering from visual sharpness and objects may appear blurry. Fortunately, most children will outgrow this condition.
Myopia vs. hyperopia
A (myopia) nearsighted person sees near objects clearly, while objects in the distance are blurred. A (hyperopia) farsighted person sees far objects clearly, while closer objects are blurry.

Myopia (nearsightedness) – Near = Clear / Far = Blurry
Hyperopia (farsightedness) – Far = Clear / Near = Blurry
Astigmatism (blurred vision)
First of all, take a peek at this image and you’ll get a quick review of the anatomy of the eye. It’s a pretty amazing organ, the eye!

Do you see that clear-like membrane in the front part of the eye? That is the cornea. It is the transparent part that covers the iris and the pupil. Think of a camera lens. I will often put a protective filter over the end of my lens. The cornea is kinda and sorta like that. If I put a protective, clear covering over my lens and the covering’s glass is not as perfect as the glass in my lens, then my images may be a bit distorted. Likewise, I may have a lens with an imperfect piece of glass on the inside. Too, my image may be a bit distorted.
Like a camera lens, our eyes may have a bit of a distortion to either the cornea or the lens. And, as a result, we may “see” a distorted or blurry “image.”
It would kinda be like looking through that old lead glass; the images seen on the other side of the glass are not “seen” clearly. They are blurry or somewhat distorted.
There are two kinds of astigmatism:
- Corneal astigmatism – The cornea may be misshapen.
- Lenticular astigmatism – The eye’s lens may be misshapen.
Astigmatism is what I discover most often during my school house screenings. Teachers will notice the child may be squinting in order to try to “adjust their aperture” and to see clearly or they may have a headache after a day of “trying to see good” (eyestrain). Children are less likely to complain of the vision issue because, to the child, it may be the normal.
Another observation I have made is: Often, when we discover the possibility of astigmatism, when calling the biological parents, the parents or another close relation will have astigmatism as well.
Tip: Seldom is astigmatism referred to as “an astigmatism.” It’s usually just astigmatism. And, it’s not “a stigmatism” as if the word “a” is being used as an indefinite article and “stigmatism” is the condition being discussed.
Anisometropia (unequal refractive power)
Anisometropia: an·iso·me·tro·pia | \ ˌa-ˌnī-sə-mə-ˈtrō-pē-ə\ – Truth be known…I have a heck of a time pronouncing anisometropia…heck of a time. Shoot! I have a heck of a time pronouncing many “medical” words. Here in Idaho I can “wing it” and then blame it on my “Southern tongue” not being able to “wrap around it.” Then, when we had a brief moment in Tennessee I told a pharmacist that “I had a hard time” with a word because “I am from the South and couldn’t wrap my tongue around it.” He didn’t laugh. He responded, “What are you talking about? I’m from the South too and I say it just fine.” Tennessee? South?? Hummm….if you say so.
Man! Do I know how to digress or what?!
Anisometropia is a condition when the eyes have different refractive power. But, what does that mean? Refraction of light is how the light “bends” when it “changes direction” after passing through a particular medium. Sort of like when light hits the surface of the water and it changes just a bit.
Our eyes…well…the lens, cornea and all that light passes through bends and it bends on purpose; it’s supposed to in order to “bend” toward a single focal point. The light is supposed to “bend” the same in each eye. But what if only one eye has myopia or only one eye has hyperopia? What if one eye has myopia and the other eye has hyperopia?? WOW! In any of these three cases, the child may have a condition called anisometropia.
We use both eyes together. That’s called binocular vision. If anisometropia is not corrected early enough, the brain may pick-and-choose which eye to “see from.” Sure, the child will still “see” from both eyes. However, the use-it-or-lose-it phenomenon may develop. Eventually the visual cortex of the brain will not use one of the eyes “as much” and a condition called amblyopia (lazy eye) may develop.
Strabismus (eye misalignment)
Strabismus, to put it simply, is when the eyes point in different directions. Another name for strabismus is not one of my favorites because of the teasing I used to hear on my elementary school’s playground years ago. Cross-eyed or wall-eyed are two other names for strabismus. One eye may look straight ahead while the other eye may turn in, out, up, or down. And later, the eye looking straight before may be turning cattywampus.

You may even see the term “gaze” to describe potential muscle misalignment of the eyes.
In normal vision, the brain institutes the six eye muscles to work in tandem to move the eyes together in order to “look” in the same direction and see a three dimensional image of the environment. This also gives us depth perception. When the child has this condition, the child’s visual cortex will “ignore” one of the two images coming into the eyes and, consequently, the child loses their depth perception. You’ll likely see this condition in children with Downs Syndrome (among other brain disorders).
Most of the time, when screening for children, I don’t even see the misalignment of the eyes; it is just so slight. Nonetheless, I suggest to the guardian that they seek the advice of ophthalmologist (eye M.D.) or optometrist.
Anisocoria (unequal pupil size)
In photography, light enters the camera through the lenses, then the iris, and then through the shutter and then onto the film / digital sensor. The amount of light that strikes the film / digital sensor is directly influenced by both the iris size (f-stop) and the shutter speed.
Now, let’s really look closely at the iris size (aperture). To put is simply, anisocoria is when our iris sizes are different (beyond a measured 0.4mm difference between pupils). The size of the pupil determines the amount of light that enters the eye (we squint when looking at bright lights in order to further reduce the amount of light that enters the eye…like a second iris). When the eye’s iris / aperture / “f-stop” are different, more / less light enters one eye than the other.

About one-fifth of the population has (yet rarely suffers from) physiological anisocoria. They’ll less than likely even know they have the difference in pupil size. But, unlike the other eye conditions, if you see a difference in pupil size after an injury, your nursey-senses should kick in and be alert for a number of possible serious conditions. Such unequal sized pupils could even be the result of coming into contact with alkaloids present in some plants.
Encourage the children to BE SAFE!
My two stepbrothers were absolute trolls to me when I was growing up. Before my mother met their father, the older of my stepbrothers, “Bucky” (11 years my senior), was hit in the eye by a bottle rocket launched by his younger brother, “Big Kevin” (9 years my senior). And still Big Kevin would shoot bottle rockets at me years and years later after “putting out” his older brother’s eye. Go figure.
Even though my older stepbrothers were mean to me…I still feel bad for all the covert revenge tactics that I deployed against them over those years. (I’m TOTALLY lying! I don’t feel bad at all.) Bucky had been known to repent at church because why else would the Good Lord cast down so many curses on him? Poor fella. But that eye…I just couldn’t tell him.
You see, Bucky’s left eye didn’t work at all. As a matter of fact, it would “point” in a different direction than his other, “good” eye. “Little Kevin (that was me…and a story for another day), look at my eyes. Are they both turning together at the same time?” he would ask me, sounding a little desperate before going out on a double-date with a girl. He wanted to make sure both eyes were moving left and right, up and down at the same time. But, no… that left eye would just stay there and stare at me as his right eye moved all about.
“Yep. It’s moving. Good job.” No, it wasn’t a payback thing. It was just that… well… I just couldn’t tell him. I felt so sorry for him.
This school year, I have had a kindergartner that was shot in the eye at point-blank range with a BB gun. What was that older sibling thinking?? He wasn’t. She almost lost the sight in that eye. And, thank goodness that incident nor that BB gun was at school.

I hope you enjoyed this article. There’s more coming. Want to make sure you get the latest from your ol’ buddy Nurse Kevin? Sign up for the Go See The Nurse Newsletter (I won’t bug you; I promise).
Your information is kept private! Here’s my Privacy Statement.