

My school district has some of school nursing’s best-of-the-best-of-the-best school nurses. Ain’t none of them ever punched me in my nose, and ain’t none of them called me “male nurse”…too often. The other day, during our meeting, we talked about a lot of things (which is what folks usually do during a meeting). One topic was the district’s policies and procedures specific to us school nurses when it comes to caring for the children from screenings for pediculosis to screening for scoliosis.
The question presented by the group was: “Should scoliosis screenings be something we school nurses do during the school year?” We were all asked to reflect on and plan on discussing this topic during our next meeting.
We may not get fully into ‘what is scoliosis’ in this article, but we will talk a little bit about scoliosis screening. When it comes to children, we’ve known “forever” that early diagnosis and prompt treatment can mitigate a bit of misery in their little world (both present and future). Back in the early 1960s, an orthopedist named G. Dean MacEwen, MD encouraged schools to institute a scoliosis screening program. It makes complete sense, right? A large number of young children are all concentrated at the same place and at the same time. Why not screen the “gathered” high-risk population and get the biggest bang for the buck?
Despite the initial intention of districts across the country in implementing in-school scoliosis screening back in the ’60s, as time went on, these screening programs have gone the way of the dodo bird. But why? To put it plainly: It’s likely due to a lack of supporting data showing that there is minimal harm (as well as cost-effectiveness) to those being screened. That’s not a personal bias; there are just so few studies that show:
- That children with scoliosis-like symptoms would be “missed” altogether if an in-school screening program did not exist.
- That scoliosis screening in school effectively identifies the children with scoliosis AND those without scoliosis (later we’ll talk about the false positives and the false NEGATIVES).
If you’re saying “shame on Nurse Kevin for saying ‘cost-effective’ when it comes to the children.” Hang on to that hate email; I ain’t the one payin’ the bills around here and surely ain’t the one making decisions. Politicians and policy-makers look at cost in making policies…period! If the cost cannot be justified, they will likely not support it. What I am saying is that the “supporting data” that in-school screenings are cost-effective does not exist to the extent where a “finger can be put on the number.”
I grew up in the ’70s and ’80s; I have no memory of having been screened for scoliosis at school. I am sure I was screened at the one of many regular pediatrician appointments that my mother diligently took me to, though I don’t remember a screening there, either. What I remember are two things about going to the doctor’s office back in those days: 1) You had to get naked (down to the BVDs), and 2) you got a shot. I now know why we had to get naked…so the doctor could look at our backs (among other details of our birthday suits).
It’s clear that many of the children we care for at our schools are growing up in a much different “world” than we grew up in. I am not talking about the “world” in the 21st century. I am talking about children with some really broken-up little “worlds.” Some of these children go to the doctor (maybe) only whenever they are sick or injured enough to miss school and visiting whatever quick care or urgent care with an empty chair in the waiting room (a rarity in and of itself). Those PAs and NPs (and maybe an MD or DO (if you’re lucky) are very unlikely to assess for anything other than the urgent need that the parent brought their child in with. Performing an Adam’s forward-bend test is simply not going to happen.
A trick question
Is screening for scoliosis at school by the school nurse a good or bad thing? Ha! A trick question, right? Many of us will lean toward “good” as being the answer to that question. After all, “early detection” and all that, right? We screen for vision, hearing, dental, and maybe a thing or two more during the school year. Why not screen for scoliosis?
I’ve looked for a solid and substantiating study on in-school scoliosis screening that would support the benefits of in-school screening and not just the cost-effectiveness of the screening, either. Unfortunately, there are no large studies. “The current available evidence in the literature for routine scoliosis screening is low to moderate.” But what about “the one child” that got missed? What I mean is this: what if you were to assess 450 children and find one child early enough to make a difference? Would that make in-school screenings worth it? But, what about the other 449 students? How will they feel having to show their bare backs to school staff that they see everyday? What about the time involvement? Would spending time preparing the screenings, promoting the screenings, performing the screenings, documenting the findings, calling the parents, and following up with the parents be time well spent? Sure! At surface value, it would seem so. But what about a child that was “missed” because they needed the school nurse for whatever other reason (you know…the bonked heads and scuffed knees)? There’s only so many hours in a day, and saying “yes” to some usually results in saying “no” to others.
One article I ran across said, “In 1996, the U.S. Preventative Services Task Force reviewed all of the studies that had been done on the topic of scoliosis screening programs and concluded they should not be recommended. But in 2008, a task force consisting of four medical associations — the American Academy of Orthopedic Surgeons, Scoliosis Research Society, Pediatric Orthopedic Society of North America, and the American Academy of Pediatrics — issued a position statement stating that they would not support any recommendation against school screenings.” Basically, they are “in the middle.”
This article also explained that “…scoliosis screening programs help detect this deformity early, which in turn, can help prevent unnecessary back surgeries. Also, in poor or under-served neighborhoods, school-based scoliosis screenings may be the child’s only chance to get the help they need in a timely fashion.” However, screenings are just to “help identify a problem” and not “the help they need if a problem is identified.” Parents must still act in some form or fashion. Finding the problem is only the tip of the iceberg; parents in these “poor or under-served neighborhoods” may (and often will) need hand-holding guidance to find both the treatment and the resources for the treatments.
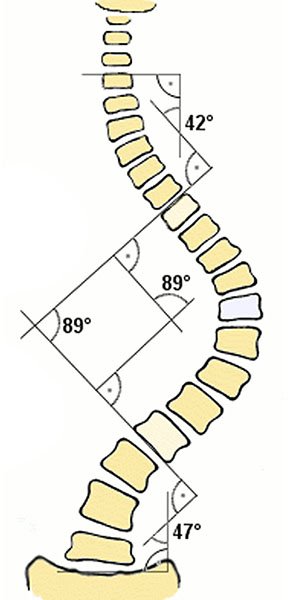
Considering the treatment standard as related to curvature (based on the Cobb Angle):
15° (give or take) = Regular check-ups are all that’s needed.
20°- 40° = A back brace (like the “Wilmington brace”) may be necessary to stop the possible progressing curvature.
Greater than 40° will result in surgery.
The study clarified this point: “448 children needed to screen to identify 1 child who subsequently received treatment.” Now, with that being said, would in-school screenings by a registered nurse who has never worked with scoliosis patients or in the orthopedic field be the be skilled enough in his or her screening to “catch” the one child out of 448 children?
Let me pause…I am not saying that we should or shouldn’t do in-school screenings; I am trying to be unbiased. Because we also have to consider the 447 other children. What about the false positives? Another perspective is: What about the false negatives? What if a child has been screened by the school nurse and the child is found not to have an issue. The parent is notified that a professional registered nurse has screened her child, and the child checked out A-OK. Would the parent’s confidence in the screening be such to where she herself would not “look” at her own child…just to make sure?
How long does it take to screen for scoliosis? 4-5 minutes? But what about organization? Every procedure starts with explaining to the patient what the procedure is and what to expect. Just turning the child around and pulling up their shirts for a look-see isn’t gonna workout very well. Many older students will ask questions. They have the right to ask questions (younger students too). There’ll be time needed for collaborating with the teachers? Providing privacy? Negotiation of clothing? Having female/male staff available to children who require same-gender faculty members to assess? Having to make sure you have a faculty member of the opposite sex (of the school nurse) trained and ready to screen those children with anxiety in showing their bare backs? What if we say that each child takes 4 minutes to screen (a conservative number)? To find that 1 child out of 448 children, we may invest 30 hours (and this is just the screening time and not the pre- and post-screening “stuff”) of pure eyes-on-spine time. Trying to assess almost 450 kids in a week would make anyone cross-eyed and surely result in both false positive…and…false negatives.
The screenings would have to be done over a period of time. I can say this: some teachers will definitely not like this at all. Teachers have a mission to accomplish each year, and they are performing this mission in an educational institution, not in a medical institution. The ultimate goal of the school and of teachers is to educate. Though the actual screening will take less than 5 minutes, would the disruption to classroom instructional flow be to the degree that a child or even children will miss some important instruction and therefore lose the benefits of what they are actually in school to receive? Apprehension leading up to the screening will affect the children’s learning for hours, if not days, before the screening. I know when I teach the “growing-up” class to the 5th-grade boys, they come in all worked up and anxious…like they’ve been all day.
Before deciding to incorporate a scoliosis screening program (or if looking to improve your scoliosis screening program) you’ll need to ensure the following:
1. Support of your teachers. Hands down! If they don’t want it to happen, your screening day will be stressful and result in loss of focus. A well-organized “why we screen” presentation for the teachers may help solidify the staff that are supportive of in-school screening and gain the support of those that are more oppositional…for lack of a better word.
2. Plan to screen about 5-10 students an hour as well as “man the fort” personnel like a substitute if you, the school nurse, are doing the screening. Consider the cost! If the nurse is screening all day, who will see the children that will be visiting the health office? What about the emergencies? A substitute school nurse? Yep. That’s my second choice. Consider the cost of the substitute nurse and the cost of a certified group of professionals trained in identifying possible scoliosis-like issues.
3. A dedicated space will need to be established and maintained during the screening process. You MUST ensure this space provides privacy. You’ll need this space TIMES TWO (x2)…boy-girl, right?
Boys may need to strip to the waist and wear briefs or gym shorts (and not the Army-style line up either [trust me…that was humiliating, to say the least]).
Girls may need to wear swim suit tops or sports bras on screening day.
Each child needs a disrobing area separate from the screening area and separate from the re-dressing area. If you’re asking why I think they should not be required to undress and re-dress in a gym-like area, consider the “awareness” of the screening. Boy and girls who are trying to get dressed and may very well have a curvature of the spine may be pointed out by and teased by a knucklehead peer (Yeah! Knucklehead!). Just dressing out for PE is one thing, but now that the focus is on seeking physical abnormalities, children are keen on pointing out the “splinter in their classmate’s eye.” “Look at Tommy’s back. It looks like a snake! Ha Ha Ha!”
The child may need to stand barefoot on the floor. Mats will work great for both sanitary reasons (I’m not planning to stand barefoot in a public building, either). The mat will provide an identifiable place for the child to stand during the screening.
Light…don’t forget that the screener will need to have great (not just good or adequate) lighting.
4. Like I mentioned before, pre-screening explanation/teaching is never to be underestimated to facilitate a positive screening experience (not to mention compliance of the procedure). Having images of the screening process or even short videos to show the children that are a bit more apprehensive than…well…they’ll ALL be a bit apprehensive.
5. Have a policy regarding notification for parents and guardians to ensure compliance in seeking care AND resources for those families that need help in paying for diagnosis and subsequent treatment. We school nurses will need to inform the children’s guardians where to go for an official diagnosis and treatment plan. We school nurses need to know what community resources are available for further diagnosis and treatment, the follow-through process, and possible educational accommodations. You may show them the finish line, but if they ain’t got no shoes to run in…they will not run this “race.”
6. Establishing an age group to screen. Scoliosis Research Society has recommended annual screening of all children aged 10-14 years. The American Academy of Orthopedic Surgeons has recommended screening girls at 11 and 13 years and screening boys at age 13 or 14 years. The state of California requires scoliosis screening for girls in the 7th grade and boys in the 8th grade; early detection should still be considered the name-of-the-game. Keeping an eye out for all children and offering yearly screenings for willing parents and children in grades between 5th and 10th would be most beneficial.
Here’s what Nurse Kevin thinks:
If the budget allows, an outside organization could be invited into the school to screen the children. If your community is fortunate, the screening team may volunteer their services at no charge to the school/district. A bona-fide, certified team of scoliosis-screening gurus would be perfect for “catching” those bendy little spines. These guys know what they are looking for.
With a team of pros, the number of false positives would be reduced. This would reduce the needless follow-up care and time commitments of the guardians (time being something in short supply with many parents; they are just like you and me: BUSY BEING BUSY!). It would also reduce the time missed in school by the student that needs follow up based on the suggestion of the screener of the (what turned out to be a) false-positive screening findings. Keeping children in school; that’s the ultimate goal of the in-school screening program in the first place, right?
With a team of pros, the number of false negatives would be reduced. This would reduce the delay in care for these children…and that’s the ultimate goal of the in-school screening program.
Consider the dental team that comes to our schools every other year and performs exams and very minimal treatments on the children’s teeth. They are a wind-up-and-go team that is highly organized and efficient. Using this model to screen for scoliosis in our school’s population would be an idea to consider.
If there is no outside organization, the school nurse could be trained by an orthopedic professional and have a bit of clinical time in assessing for scoliosis under the direction of this pro. Only a day of instruction and practice…maybe two days…should be sufficient (no less than about 4 hours). And, the school should have both a male and female screener. Maybe a female nurse (usually the case) and a male coach (also common). At my school, there’s me and my “Y” chromosome and our awesome school PE teacher, who sports a duel “X” pair of chromosomes. We’d be a perfect back-checking team.
Permission forms should be sent home as should instructions on both what the screening includes AND simple-to-understand instructions on how to assess for scoliosis on their own for their own child. THIS would be the biggest part of screening…empowering the parent and creating parental awareness of scoliosis. And yes, some would check….and…no…some would not. Remember that parent who said they “always check for head lice?” Remember that parent who said told you last year that they’d get that last MMR vaccine by the first of the next school year?
Okay. Okay…
We’ve talked about a lot of issues regarding scoliosis screening in schools. We know that parents are busy being busy. We school nurses and teachers may kinda-sorta feel the parents should be tending to the health maintenance of their own children. But, truth be known, many do not see to (or are unable to address) their child’s basic healthcare needs. Think about how many children in your school that are not fully immunized for whatever reason. How about the child with many, many dental caries and other issues discovered during an in-school dental exam? I am not suggesting these parents are bad parents; not at all. I am suggesting that some parents just need a bit of help (if not for the parent but for the little person “in the middle”)…and we school nurses need to be that help. We are not just school nurses…we are community-health nurses.
So, in-school scoliosis screening? Sure! It’s a good idea. If we “catch” the one child out of 448 children who may have a slight curvature that could be corrected with a brace early on, we may end up helping a child live a life without visible deformity, without emotional distress, without intractable pain, and without possible organ dysfunction? That’s what Nurse Kevin thinks. What do you think?
To sum this up:
Permission forms should be signed by the guardian to avoid having the child assessed who is already undergoing cares for scoliosis or other orthopedic issues (and to avoid the “why” questions afterwards and the time spent screening).
Both a male and female screener should be available.
Screenings should be done by a team of professionals that know just what to look for. Our local community should be welcomed into our schools with their desire to support the educational needs and health needs of the children (and NO…not just by raising taxes, either [did I just get political…wow…that’s not like me]).
The screenings should be scheduled after the Christmas break. Why? Do I really have to ask you how busy you are in August and September with enrollment, allergy tracking, and immunizations? Na, you ain’t busy in October and the first of November trying to schedule flu shots for children and staff. And, I would not dare schedule scoliosis screening between Thanksgiving and Christmas breaks.
Funny thing about permission forms…sometimes parents don’t remember filling them out. Sometimes the ex-spouse with differing healthcare perspectives will fill out the form just to “poke” at the other parent. And permission forms will usually avoid the “why questions” that always pop up afterwards. I don’t get permission forms for eye screenings and do not plan to start for this screening specifically. Nonetheless, I get calls, “Why did you check my Tommy’s eyes without my permission?” I wish this was not such a big issue for so many parents…permission forms, that is. Imagine giving a child a vaccine without a permission form. WOW! That parent will come down on you like a tornado with teeth and fingernails! You’d likely lose your job (but no one would ever ask the parent why, “Why didn’t you immunize your child in the first place? This nurse helped you out by giving your kinder the last DTaP and kept you from being a law-breaker.” Truth-be-known…I absolutely prefer permission forms, not only for liability issues but also to help me, the school nurse, know exactly what the parent’s wishes are for their child. I’d expect the same understanding from my child’s school nurse (only my child’s school does not have a school nurse…hummmm…).
Here we are, almost 3,500 words later, and I still have not talked about scoliosis itself, nor have we talked about the different screening methods. Those topics are entire articles in and of themselves, as well as being beyond the scope of this article. So, let’s call it a day. Be sure to add your comments below…agree or disagree or other: To Screen Or Not To Screen.
May Your Backs all be Unswerving,
Nurse Kevin


Intriguing article. You had to get naked (down to the BVDs) did rather confuse me- I assume it may relate to underwear but finding an unfamiliar term I looked it up. Bovine Viral Diarrhea eh- made me laugh. (I’m English so never heard of BVDs) Thanks for the laugh though in an otherwise tough day school-nursin’
Ha! BVDs…yep…a reference to underwear (a brand called BVDs…kinda like Fruit of the Looms). Are you in England? I am glad you got a good laugh…I had “one of those days” yesterday too.